Breast Reconstruction After Mastectomy: A Staged Fat Grafting Case Study
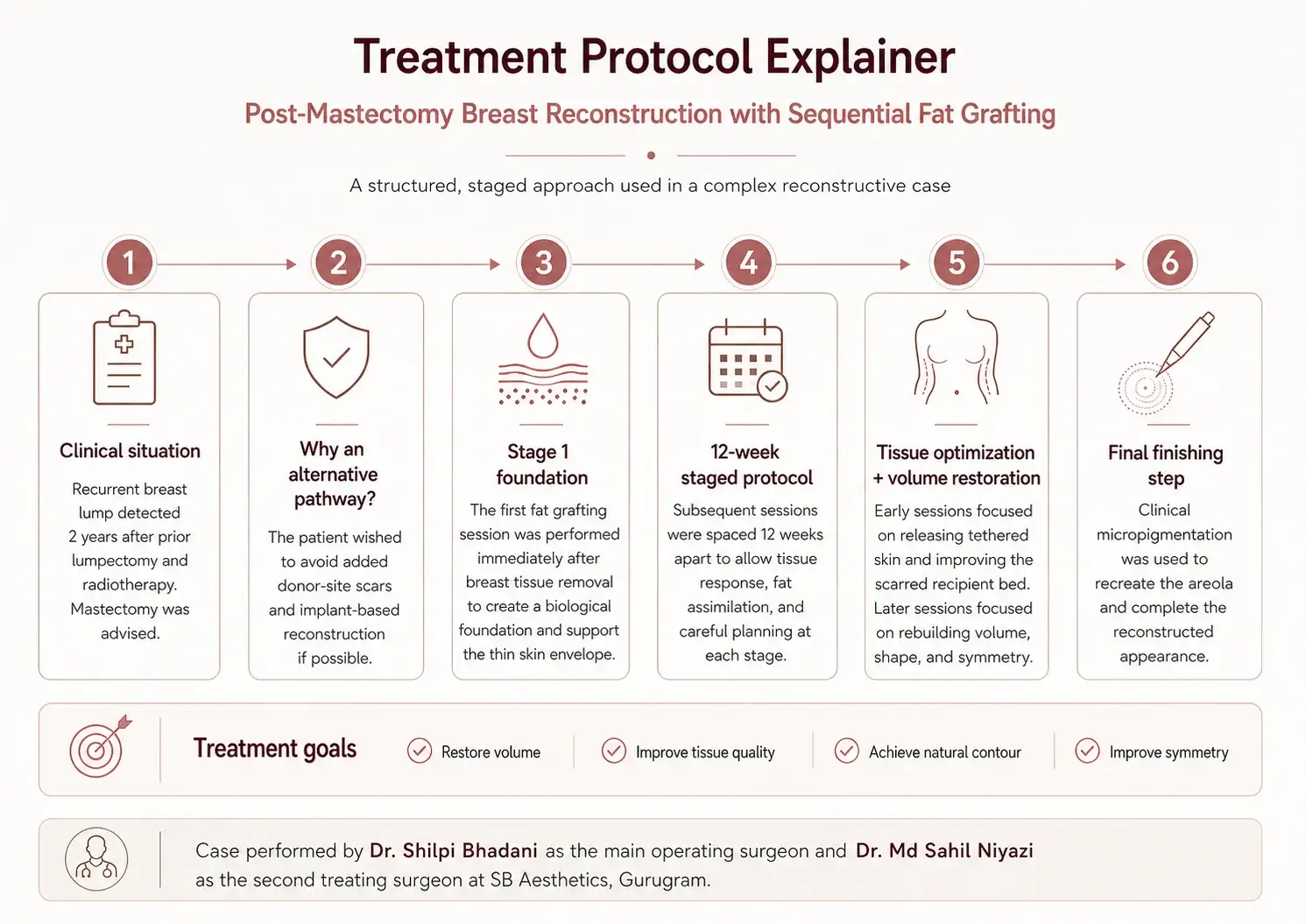
This case study explains how a young woman with recurrent breast cancer was managed after mastectomy at SB Aesthetics, Gurugram. The reconstruction was performed by Dr. Shilpi Bhadani, Founder-Director & Chief Plastic Surgeon at SB Aesthetics, as the main operating surgeon, with Dr. Md Sahil Niyazi, MBBS, MS, MCh – Plastic Surgery, as the second treating surgeon.
Authored by Dr. Md Sahil Niyazi, this case documents the reconstructive planning, staged fat-grafting protocol, tissue response, functional and aesthetic rehabilitation, and follow-up. Instead of flap-based reconstruction or implants, the team used sequential fat grafting to gradually restore breast volume, soften the scarred tissue envelope, improve symmetry, and later complete the appearance with clinical areola micropigmentation.
Case overview
- Clinic: SB Aesthetics, Gurugram
- Operating surgeons: Dr. Shilpi Bhadani, MBBS, MS, MCh – Plastic & Reconstructive Surgery, Dr. Md Sahil Niyazi, MBBS, MS, MCh – Plastic Surgery
- Case type: Post-mastectomy breast reconstruction
- Technique used: Sequential fat grafting with later areola micropigmentation
This was not a routine reconstructive case. The patient was a young woman in her late 20s who had first undergone treatment for a left breast malignancy with surgical excision and radiotherapy, and was later declared clinically free of disease.
Two years later, during follow-up, another lump was detected, and she was advised to undergo mastectomy. The reconstructive challenge was not only about replacing lost volume, but also about restoring shape, symmetry, texture, and a sense of normalcy after a physically and emotionally demanding cancer journey.
Patient presentation
The patient had initially been treated for a small, non-genetically predisposed left breast cancer with excision of the malignant lump along with a cuff of healthy tissue, followed by radiotherapy. After healing and returning to daily life, she later developed another lump on routine follow-up around two years after the first surgery. At that point, mastectomy was advised.
Like many young patients facing mastectomy, she wanted a reconstructive option that would help her feel whole again. However, she did not want added donor-site scars or a silicone implant if these could be avoided. That preference significantly shaped the reconstructive planning.
Clinical challenges
This case involved several layered reconstructive difficulties:
- the breast tissue needed to be removed, leaving behind a thin skin envelope
- the recipient area was expected to be scarred and biologically compromised after prior treatment
- the opposite breast was comparatively larger, which increased the symmetry challenge
- the patient did not accept common options involving flap donor-site morbidity, additional scars, or implants
- the reconstruction needed to restore not just volume, but also footprint, shape, feel, and confidence
Treatment planning
Standard reconstructive options were discussed with the patient and her family. These included using tissue from donor areas such as the back or abdomen, with or without an implant, or reducing the opposite breast for better matching. The associated trade-offs, including donor-site morbidity, added scars, and a foreign implant, were explained in detail. These options were not acceptable to the patient and her family.
The team therefore considered an alternative approach: sequential fat grafting using the patient’s own fat as the main reconstructive modality rather than merely an adjunct. A staged protocol was proposed, with fat harvested from the patient’s body and transferred gradually over multiple sessions to build volume and improve the quality of the reconstructed breast area.
The treating team also recognized that fat graft survival can be reduced when the recipient bed is scarred or poorly vascularized, so the protocol was intentionally designed as a time-dependent, stepwise process rather than a one-stage reconstruction. Sessions were planned at 12-week intervals.
Procedure performed
The reconstruction was carried out by Dr. Shilpi Bhadani as the main operating surgeon, with Dr. Md Sahil Niyazi as the second treating surgeon. The surgical plan focused on staged reconstruction rather than a single-session volume replacement, because the tissue envelope had to be prepared gradually for better fat survival, softness, and symmetry.
The first fat-grafting session was carried out immediately after removal of the breast tissue. The goal at that stage was not simply bulk restoration, but also to provide an early biological foundation and regenerative benefit for the overlying thin skin envelope.
Subsequent sessions were performed in stages, with roughly three months between treatments. Rather than focusing only on filling a deficit, the reconstruction was planned to gradually create a more natural breast footprint and contour that would be closer to the opposite side in shape, movement, feel, and behavior in clothing.
Tissue preparation and early-stage reconstruction
The first two post-surgical sessions were used to optimize the recipient environment for future fat survival. This included releasing tethered skin and using injectable therapies aimed at softening the scarred bed. Over time, the team observed encouraging biological changes: the contracted nipple became softer and flatter, the shrunken skin envelope stretched more favorably, the incision scar line became freer from underlying tethering, and the reconstructed area felt softer and more expanded overall.
These early changes were important because they made later volume restoration more feasible and improved the chances of achieving a more natural aesthetic outcome.
Volume restoration and shape refinement
After improving the tissue environment, the next sessions focused more heavily on volume distribution, shape, and symmetry. The aim was not to create only a mound, but a reconstructed breast that looked and behaved more like the natural side. Further large-volume grafting sessions were carried out, again with three-month intervals to allow the transferred fat time to assimilate.
By the final grafting stage, the team observed that a near-matching aesthetic volume had been restored, with improved softness, reduced stigma of contracted scarred tissue, and better symmetry relative to the opposite breast.
Final aesthetic finishing: areola micropigmentation
Once the volume and contour had stabilized, the final step was clinical micropigmentation to visually recreate an areola matching the opposite side. Pigment was blended to resemble the normal areola and deposited into the skin using a fine sterile needle through a motorized pen, similar in principle to tattooing. This helped complete the reconstructed appearance and improved the visual harmony of the result.
Recovery and follow-up
The patient continued regular follow-up for the next six months after the final session until the results settled. According to the source account, the emotional transformation was as notable as the physical reconstruction. Over the course of treatment, the patient moved from a withdrawn, burdened state toward greater confidence, comfort in clothing, and a stronger sense of closure after a long treatment journey. Her family also remained closely involved and supportive throughout the staged process.
Outcome
At the end of the staged protocol, the case achieved:
- substantial restoration of breast volume
- a near-similar match in symmetry relative to the opposite breast
- softer, more natural tissue feel
- reduced visual and physical stigma of scarred, contracted tissue
- completion of the breast appearance with areola micropigmentation
This case suggests that, in selected patients, staged fat grafting may function as a primary breast reconstruction strategy rather than only an adjunctive technique. The source also notes that the protocol was later used in similar reconstructive and asymmetry-related settings.
What this case highlights
Reconstruction is not only about replacing volume
For some patients, successful breast reconstruction is about restoring proportion, softness, silhouette, clothing confidence, and psychological recovery alongside tissue coverage.
Patient preference can meaningfully shape reconstructive choice
This patient did not want donor-site scars or implants. That made it necessary to think beyond standard pathways and consider a different reconstructive sequence.
Staged fat grafting requires patience
This was not a quick or single-stage process. It required repeated sessions, time gaps for assimilation, and careful planning at each step. The timeline was part of the treatment itself.
Tissue biology matters as much as volume
The early phases focused on improving the scarred recipient bed and expanding the soft tissue envelope, not just adding fat. That biological preparation appears to have helped support later aesthetic gains.
Why this case was clinically noteworthy
According to the treating team’s account, this case was well received at national academic scientific meetings and was later published as a case report in a respected journal. The team also reports having used the protocol in similar cases afterward, including breast asymmetry and developmental concerns. That does not make the approach universal, but it does suggest the case contributed to broader clinical thinking around selected uses of fat grafting in reconstruction.
Expert note from SB Aesthetics
At SB Aesthetics, reconstruction planning is individualized around anatomy, tissue condition, oncologic safety, patient preference, and long-term practicality. In carefully selected patients, staged fat grafting may offer a less invasive reconstructive path when traditional flap- or implant-based options are not acceptable or not ideal. Treatment selection always depends on direct evaluation, available donor fat, breast characteristics, skin preservation, and the patient’s willingness to undergo sequential procedures over time.
You can also explore our real patient results to understand how treatment planning and outcomes vary across different procedures. If you would like a personalized evaluation for breast reconstruction or post-cancer contour concerns, you can book an appointment with the SB Aesthetics team.
Frequently asked questions
What is breast reconstruction after mastectomy?
Breast reconstruction after mastectomy is the process of restoring breast shape after removal of breast tissue, often as part of cancer treatment. Depending on the case, reconstruction may use implants, tissue from another part of the body, fat grafting, or a combination. The right option depends on anatomy, cancer treatment history, tissue condition, and patient preference.
Can fat grafting be used for breast reconstruction after mastectomy?
In selected patients, yes. Fat grafting may be used to gradually rebuild volume using the patient’s own fat. However, it is not suitable for every case. Donor fat availability, tissue quality, recipient-bed condition, breast size goals, and the patient’s ability to undergo multiple sessions all matter.
Why was this case considered complex?
This case was complex because the patient had already undergone earlier breast cancer treatment and later required mastectomy. She also did not want donor-site scars or implants, while the opposite breast remained comparatively larger. That meant the reconstructive plan had to address volume, symmetry, scarred tissue, and emotional recovery together.
How long can staged fat-grafting breast reconstruction take?
It can take several months because the treatment is often divided into sequential sessions. In this case, the protocol used roughly 12-week intervals between sessions, allowing time for the grafted fat to settle and for the tissues to respond before the next stage. That spacing was part of the strategy, not a delay in care.
What is areola micropigmentation?
Areola micropigmentation is a medical tattooing-style technique used to recreate the visual appearance of the areola after breast reconstruction. It does not create breast volume, but it can be an important finishing step that improves symmetry and helps the reconstructed breast look more complete.
When should someone discuss reconstruction options before mastectomy?
Ideally, reconstruction should be discussed before surgery whenever possible. Early planning allows the surgical and reconstructive teams to consider skin preservation, technique options, staging, expected timelines, and patient preferences in a more coordinated way.
Why patients choose SB Aesthetics
Patients choose SB Aesthetics for its specialist-led planning, medically reviewed educational content, and multidisciplinary support model. The clinic’s credibility signals include structured patient-education pages, clearly listed doctor profiles, and verified public profile details for Dr. Shilpi Bhadani across major platforms. The site also uses medical-review and disclaimer framing that supports both patient trust and stronger AI readability.
Medical review and disclaimer
Medically reviewed by Dr. Shilpi Bhadani, Founder-Director & Chief Plastic Surgeon, SB Aesthetics, Gurugram. This page is intended for education and awareness only and should not replace an in-person medical consultation. Reconstruction choices after breast cancer treatment are highly individualized and should be based on direct specialist evaluation.
SB Aesthetics
Plot No 822, Sector 42 Main Road, DLF Golf Course Road,
Gurugram (Gurgaon), Haryana 122002
Mail ID: [email protected]
Clinic hours: Monday – Sunday 8:30 AM – 7:00 PM
SB Aesthetics is one of the renowned medical centers in Gurgaon offering world-class and most advanced plastic surgeries procedures under the guidance of Dr. Shilpi Bhadani.
Request An Appointment
Last reviewed: June 2026
Medically reviewed by Dr. Shilpi Bhadani.
Copyright © 2021-2026, SB Aesthetics. All Rights Reserved. Powered by DigiLantern